
To whose advantage is Medicare Advantage? Part 1

Note: Enrollment in Medicare Advantage plans is poised to surpass enrollment in traditional, fee-for-service (FFS) Medicare in 2023. MA's rapid growth raises major questions about the shape of Medicare coverage going forward. This is the first of two posts examining the pros and cons of Medicare Advantage. This post outlines the major issues as framed by MedPAC and select researchers, along with the basic economic tradeoffs for enrollees. Part 2 will report the experience of a hospitalist, brokers, and various stakeholders who responded to a CMS request for feedback about the MA program.

There is a slipknot quality to attempts to compare the value and utility of traditional, fee-for-service (FFS) Medicare and Medicare Advantage.
Medicare Advantage plans generally place bids to CMS far below CMS benchmarks, which are based on an adjusted estimate of what it costs to provide FFS Medicare to enrollees in the plan's geographic area. On average, according to the 2022 MedPAC report, MA plans spend 15% less to provide Part A and B benefits than FFS Medicare would spend. But CMS pays Medicare Advantage plans an average of 104% of what it would pay for FFS Medicare coverage for the same enrollees. But MA plans use the excess payment to provide an estimated $2,000 per member in surplus benefits or out-of-pocket cost release. But, according to MedPAC, the value of MA-furnished extra services as actually used by enrollees is elusive, because of inadequate reporting requirements, and the quality ratings that increase payments to MA plans do a poor job measuring quality.
With regard to outcomes, MA plans employ treatment protocols that do minimize some so-called low-value care and, in some cases at least, boost usage of preventive care that, according to some studies, can reduce cardiac events, foot amputations for diabetics, ER trips, hospital admittances, and other services. But there is also good evidence that MA plans inhibit or impede access to needed or high-value care, introduce expensive and sometimes dangerous bureaucratic hurdles to obtaining needed care, and drive enrollees with intense medical needs back to FFS.
Most notoriously, by multiple accounts, MA plans often impede, block, limit options and reduce the duration of post-acute care. Comments about MA that CMS recently solicited from stakeholders detail these complaints (from physician and hospital associations, practitioners, acute care personnel, patients, brokers and others) again and again and again. A major strain in these complaints is from state employees forced into MA plans by retirement benefit packages.
This month, the Kaiser Family Foundation published a report, based on a literature review of 62 studies published since 2016, comparing "Beneficiary Experience, Affordability, Utilization, and Quality in Medicare Advantage and Traditional Medicare." The authors' conclusions are...inconclusive:
We found few differences between Medicare Advantage and traditional Medicare that are supported by strong evidence or have been replicated across multiple studies. Both Medicare Advantage and traditional Medicare beneficiaries reported similar rates of satisfaction with their care and overall measures of care coordination. Medicare Advantage outperformed traditional Medicare on some measures, such as use of preventive services, having a usual source of care, and lower hospital readmission rates. However, traditional Medicare outperformed Medicare Advantage on other measures, such as receiving care in the highest-rated hospitals for cancer care or in the highest-quality skilled nursing facilities and home health agencies. Additionally, a somewhat smaller share of traditional Medicare beneficiaries than Medicare Advantage enrollees experienced a cost-related problem, mainly due to lower rates of cost-related problems among traditional Medicare beneficiaries with supplemental coverage. Several studies found lower use of post-acute care among Medicare Advantage enrollees but were inconclusive as to whether that was associated with better or worse outcomes. Findings related to the use of other health care services, including hospital care and prescription drugs, and condition-specific quality of care measures varied – likely due to differences in data and methodology across studies.
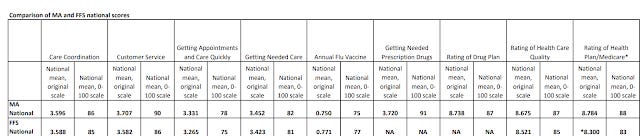
Consumer assessments of the care they receive in MA and FFS Medicare, recorded in the CAHPS survey that is integrated into quality ratings for MA plans, also suggest an overall wash across multiple measures:
Beyond the question of whether Medicare enrollees have been better served by FFS Medicare or MA to date -- or of whether the choice itself is a boon, or whether MA has yielded value for taxpayer dollars -- questions as to the future course and impact of the program are now urgent. These questions include the impact of the faster-than-expected growth of MA, in which total enrollment will surpass that of FFS in the next year or two, bringing the viability of FFS Medicare as a pricing benchmark (set by government fiat) into question; the flood of investor money into MA; the metastasizing of often deceptive advertising and marketing in MA, and its richer compensation of brokers than Medigap policies provide; faster growth in MA spending than in FFS, and a widening gap in risk adjustment scores between MA and FFS that partly drives that spending; and the impending infusion of MA managed care techniques into FFS Medicare via the ACO Reach program.
Underlying the questions raised by these developments is the meta question: does private-sector management of healthcare claims, and/or of healthcare delivery, improve healthcare outcomes and provide more value for taxpayer dollars if the "managers" are incentivized to keep per-enrollee costs down? If so, does the profit motive, unchecked as it is in the U.S. compared to other wealthy countries' healthcare systems, undermine the efficiencies the private sector may deliver? While many wealthy countries offer universal healthcare via private insurers, most put tight constraints on the arenas in which insurers can earn profits -- e.g., in supplemental insurance only, as in Medigap.
For new and relatively healthy Medicare enrollees, if they are not dual eligibles who have all or most of their premium and out-of-pocket costs paid, the choice between FFS Medicare and Medicare Advantage often boils down to: pay now for FFS (via premiums for Medigap and Part D on top of the Part B premium) or pay later in MA (via higher out-of-pocket costs, limited choice of providers, and impediments to care imposed by prior authorization).
Most MA enrollees (65% in 2021, according to KFF) pay only the $170/month Part B premium for a package deal that includes Part D prescription drug coverage and extra services, often including varying degrees of dental, hearing and vision coverage, as well as out-of-country coverage. Some retiree benefit plans pick up the Part B premium as well. MA plans also include an annual cap on out-of-pocket costs in Parts A and B, which in 2022 can be as high as $7,550 for in-network and $11,300 for out-of-network care.
FFS enrollees who buy Medigap policies generally pay $300-400 per month for Parts B, D and the Medigap policy combined. In exchange, they get all-but-unlimited choice of providers, freedom from prior authorization for almost all services, and comparatively minimal (in Plan G, truly minimal) out-of-pocket cost exposure.
Theoretically, according to some studies, MA enrollees benefit from getting steered into high-value care, including preventive care and chronic disease management. As far as provider quality goes, the studies reviewed by KFF suggest that MA plans tend to hue toward the middle, excluding both the lowest- and highest-quality (e.g, most expensive) providers. Experientially, those who can afford higher-end Medigap coverage (or whose employers provide equivalent supplementary coverage) have the keys to the U.S. healthcare system: they can seek out the care they want, where and from whom they want it, with little to no interference, and paying little to nothing out-of-pocket. If you can afford Medigap, the purported advantages of the kind of managed care provided by MA plans are likely to seem...theoretical.
Stay tuned for some on-the-ground views as to how Medicare Advantage treatment protocols play out in Part 2.
Photo by Muskan Anand
Most of the links do not work.